LP 6&7: Examples and analogies
The design of the
tele-expertise system in a French university hospital
In 2012, the University Hospital of Montpellier (France) shifted its method of clinical documentation (e.g., patient charts and flowsheets, medication order) from a paper-based system to an EPR (electronic patient record). The hospital center is in the south of France and features approximately 2,000 beds in seventy-four different departments. Overall, the hospital staff consisting of 6,000 caregivers, 1,400 doctors (physicians, anesthetists, and surgeons), and 500 residents provides treatment to more than 235,000 inpatients and 540,000 outpatients annually. The new EPR system, which is an information technology (IT)-based enterprise wide healthcare solution was designed to support all aspects of patient care, covering medical and paramedical notes and reports, physician order entry and treatment plans, laboratory management system, operating room management system, billing, and follow-up procedures. This “off-the-shelf” EPR was implemented in 9 months with a task force of one physician, one pharmacist, three manager nurses, and 100 fulltime technicians recruited for the customization during 1 year. The EPR allows customization and configuration of patients’ records through setting of new forms, queries, and personalized views.
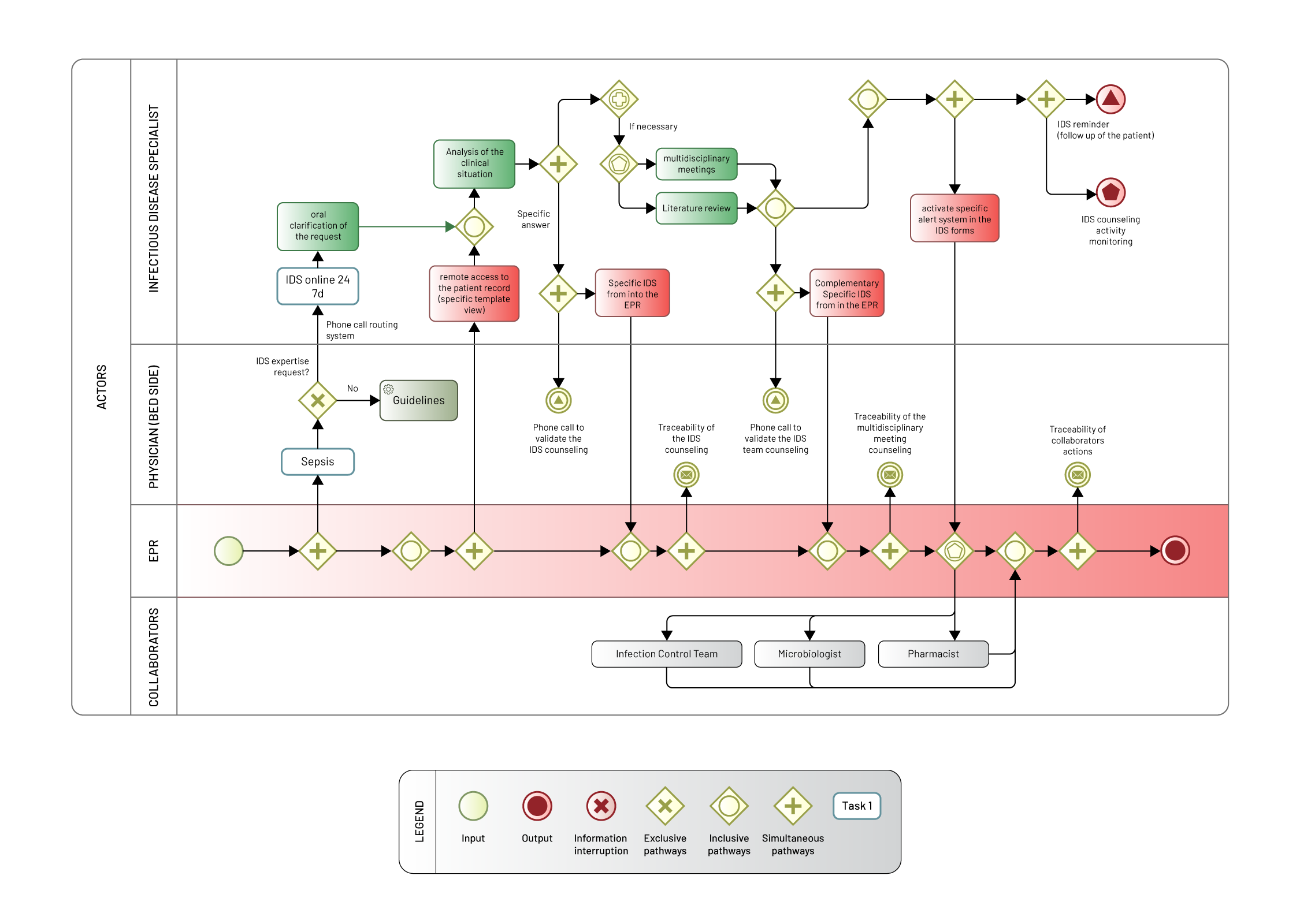
Aware of these opportunities, an IDS (infectious diseases specialist) decided to formalize the counseling activity and customize the EPR for his team. His aim is to facilitate the IDS’ daily practice of providing counsel to clinicians from every department and to increase the traceability of the activity of the IDD (infectious disease department). For this, in collaboration with the other IDS, a form was designed and deployed for the IDS initial assessment, for the re-assessment and for the decisions made during the team consultation meeting of all the IDS, the pharmacist, the microbiologist, and the infection control team. The global process is described in Figure 1. When a clinician needs more specific information than provided by standard recommendations embedded into the EPR, he or she may contact the IDS on a unique telephone number 24 hours a day, 7 days a week. A Web-based telephone call routing system is used to switch the telephone line to the IDS on call, which may change daily according to availability schedule. The requesting clinician briefly explains the medical situation and the degree of emergency and the IDS may ask for additional clarifications on the request. The call is then followed by a remote access by the IDS to the full patient’s record (including laboratory results, radiology, medical and nurses’ notes), with a specific template view (inflammation biomarkers graphs, table of microbiological results, past antimicrobial use). The information recorded includes the IDS’ previous advices, allowing follow-up care. These advices focus mainly on the diagnosis of infectious diseases or on the therapeutic use of the appropriate antimicrobial strategy, but they may also be related to the infection control issues, unexplained fever, accidental exposure to biological fluid or rabies exposure. The IDS may choose to respond make an answer alone and may justify his or her response by providing hypertext links to scientific articles. For complex cases, the clinician may decide that the response require a decision made by the team consultation meeting of the all IDS, the pharmacist, the microbiologist, and infection control team. The IDS’s response is recorded in a specific IDS form into the EPR and available in real time for all the clinicians. To enable clinicians to make medical decisions, IDS do not make any prescription, they only provide and record argued counsels. Originally, the specific IDS form was designed to record the medical reasoning and the diagnosis or therapeutic proposal, the identification details of the IDS and of the patient with a timestamp. Later, the users’ remarks and all input errors were taken into account. Consequently, all unused or ambiguous fields were removed. The information framing is based on: (a) ergonomics choices, as tabs that designate the steps of the counseling, combo boxes, checkbox, under form for the use of the typical instructions associated with dosages and monitoring of each suggested drug; (b) standardized requirements and mandatory elements, as remote or bedside assessment, allergies related to anti-infective drug, and monitoring decisions; (c) indexing of each situation by combining the clinical category of infection, the pathogens classes (bacteria, viruses, etc.), and the disease context (i.e., immunosuppression, cancer, pregnancy, etc.). The most important elements, as the analysis of the clinical situation, its history and therapeutic proposal, are described in narrative text. The size has been defined to fit the work practices of each IDS. An input help has been added. Requests have been computerized to allow monitoring of use. Furthermore, media fields have been inserted to associate an image in the form (e.g., biological result curves or patient photos) or scientific papers concerning the clinical situation. Additionally, binary radio buttons were set up linked with the automated mailing at defined time intervals (e.g., the IDS may ask for a specific pharmaceutical monitoring). The form evolved iteratively during the first year of use of the system. After, the rate of change of the form has slowed considerably with updates on the new instructions associated with treatment proposals and new ways to alert collaborators (Infection Control [IC] staff, microbiologists, pharmacists) for specific queries and to provide automatic instructions associated with the proposed antibiotic treatment. Especially, in the summer of 2015 a new feature was designed: every time the IDS completed the checkbox “alert the IC team,” a secured mail with essential clinical data is sent to the IC department. This applies to all major health-care associated infections and community-acquired infections with an epidemic potential (e.g., measles or tuberculosis). Regular automatic queries provide real-time anonymous data from IDS activity, as the number of telephone calls, the regimental number, the prescriber’s department, the infection class, the time passed since the first evaluation, and the antimicrobial suggestion. In this context, an observational prospective study was conducted to assess the diffusion of the tele-expertise system and the perceived utility for the medical managers of most demanding departments (Morquin et al., 2018).