4. Extend services through task sharing and/or differentiated care
Task sharing (task shifting) is the systematic delegation of tasks, where appropriate and allowed by health policy, to health workers with shorter training and fewer qualifications (WHO, 2008). Task sharing is a fundamental approach to promoting efficiencies and overcoming health workforce shortages or maldistribution, as less specialised workers are less costly and can be trained in less time. Task sharing implementation requires consideration of health worker's existing scope of practice and the ability to train and support them in their enhanced scope. HRH planners should also consider "the distribution of roles among cadres, regulatory issues, stakeholder involvement, training and supervision, systems for referral, supply chains, and possible changes to payments or other incentives" (WHO, 2012c).
The following are examples of how sharing selected tasks could improve health service access:
- For family planning, sharing tasks such as IUD, implant, and injectable administration among doctors, nurses and midwives expands access to modern contraception (WHO, 2017).
- For maternal and neonatal health, sharing tasks such as delivering basic emergency obstetric and newborn care with midwives expand access to safe and skilled deliveries (Deller et al., 2015).
- For HIV/AIDS, sharing tasks such as initiating and managing antiretrovirals among doctors and specially trained nurses can expand access to life-saving treatment (WHO, 2008).
- Sharing administrative tasks such as reporting or record-keeping with non-clinical staff can free clinical staff to see more patients (WHO, 2008).
More recently, taking into account the COVID-19 crisis, a new framework was developed for task sharing/shifting called the COATS framework (Orkin et al., 2021) that can be observed in Figure 2. The framework offers a simple and adaptable solution for task sharing/shifting.

Figure 2 (Orkin et al., 2021)
Differentiated service delivery models of care, or differentiated care, are innovative ways health workers can meet client needs by reducing the workload of more highly specialised workers. Differentiated care is considered a client-centred approach that changes the frequency and/or location of client contact and the type of service delivery providers. Differentiated care may include task shifting from more specialised health workers to less specialised staff, or the frequency of consultations with clinical staff may decrease (WHO, 2008).
For example, HIV-positive clients taking antiretroviral treatment (ART) who are known to be stable, adhere to their medication and do not require frequent clinical consultations could be eligible for differentiated care. Differentiated care models for HIV services can be categorised into four types:
- Health care worker-managed groups: Clients receive ART refills in a group setting, managed by either a clinician or lay worker, in or outside the facility setting.
- Client-managed groups: Clients receive ART refills in a group setting, managed by clients themselves, usually outside the facility.
- Facility-based individual models: Clients receive ART refills without a clinical consultation.
- Out-of-facility individual models: ART refills and clinical consultations are provided outside the facility.
Like task sharing, differentiated care optimises the existing health workforce that emphasises community-based health workers.
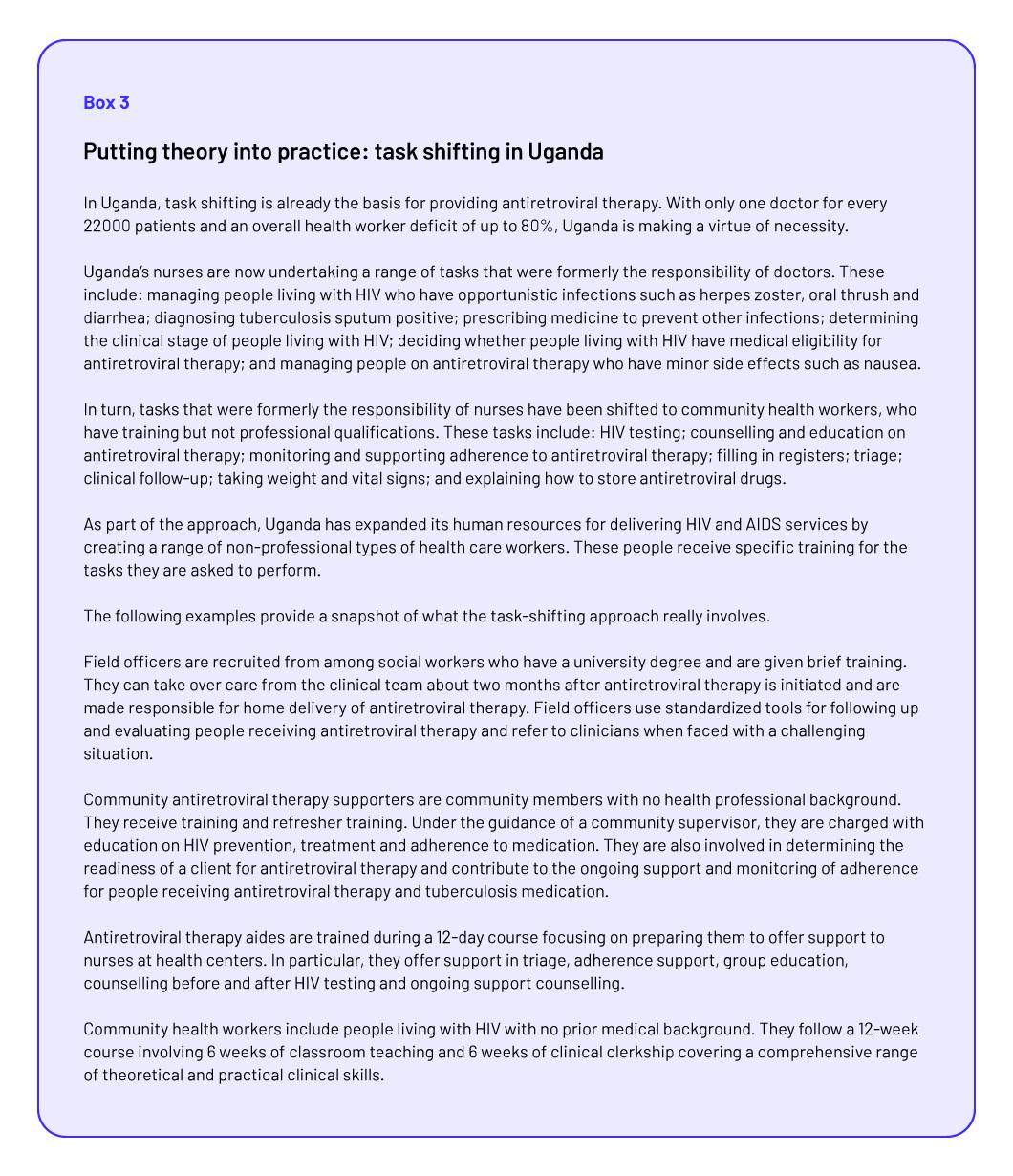
Example
for differentiated care in Figure 3 – Box 3 (WHO, 2007b):